Effective personal protective equipment (PPE) is critical for health care workers.
Doctors and nurses get infected in countless ways: airborne paths, via infected droplets (some estimate that a nurse touches over 1000 surfaces in an 8 hour shift), via contaminated hands touching the mucous membranes (eyes, nose, and mouth), through contaminated droplets in aerosol mists, etc. Contaminated airborne particles can stay suspended in the air and travel well beyond six feet. We can make a 4000-pound airplane fly, making 50 µm droplets float is trivially easy. Effective PPE used in Infectious Disease wards – with multiple covid patients and high viral loads – should protect from ALL infection routes.
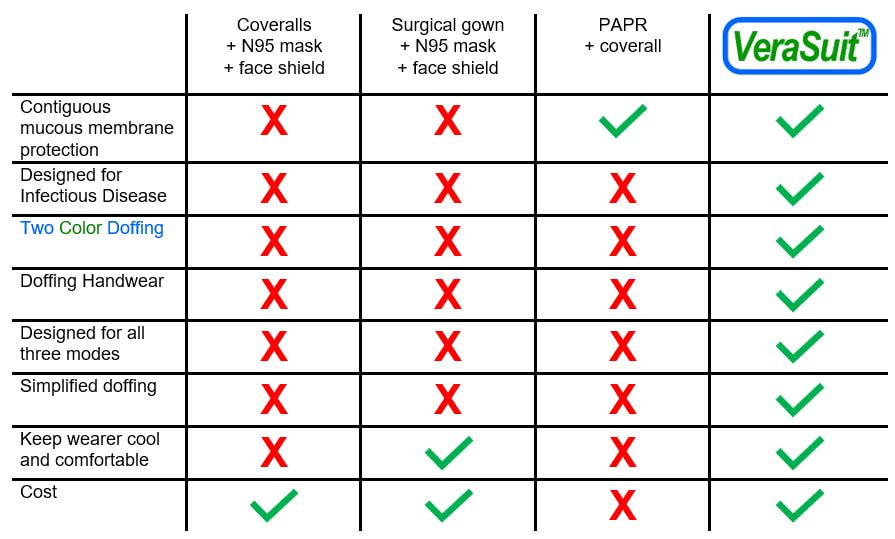
Coveralls and surgical gowns are truly miserable in this regard. The vast majority do not cover any of the mucous membranes. Frankly, these were the cheapest and widest available option on the shelf when the outbreak started. Their availability does not equate to efficacy. They rely on other pieces of PPE to cover their many shortcomings.
N95 masks are not bulletproof: they require perfect fit. If they do not create an air-tight seal around the nose, then infected air will enter through the openings around the mask (the path of least resistance is preferred in fluid dynamics) instead of passing through the filter.
The eyes also remain exposed, leaving another important entry point at risk. Face shields do block droplets and aerosols from the eyes.
Personal Air Purifier Systems (PAPRs) provide facial and respiratory protection, but these were not designed for Infectious Disease use but instead for industrial applications like silica dust. Users complain of heat, noise, and comfort, maintenance is a challenge given the many exposed reusable parts, and they were found to be so bad in doffing in Toronto in 2003 that the Ontario nurses threatened to strike if forced to use them.
Doffing is a distinguishing line between good and bad Infectious Disease PPE. There is no point in wearing PPE if the doctor or nurse gets infected removing it. Does the apparel help the wearer doff? Does it inform the user which surfaces were exposed and which were not? Does the wearer have to remove a second infected glove with a bare hand? Is the doffing simple and easy to execute? The CDC summarizes: "The manner in which the clothing is donned and doffed in sequence with other PPE is an important consideration when selecting gowns and coveralls. This is critical because the ease or difficulty with which PPE is put on and removed may affect its effectiveness and the potential for self-contamination, especially during doffing of contaminated PPE. Donning and doffing features included in the selection process should consider the entire PPE ensemble, not simply the gown or coverall."
Doctors and nurses get infected in countless ways: airborne paths, via infected droplets (some estimate that a nurse touches over 1000 surfaces in an 8 hour shift), via contaminated hands touching the mucous membranes (eyes, nose, and mouth), through contaminated droplets in aerosol mists, etc. Contaminated airborne particles can stay suspended in the air and travel well beyond six feet. We can make a 4000-pound airplane fly, making 50 µm droplets float is trivially easy. Effective PPE used in Infectious Disease wards – with multiple covid patients and high viral loads – should protect from ALL infection routes.
Coveralls and surgical gowns are truly miserable in this regard. The vast majority do not cover any of the mucous membranes. Frankly, these were the cheapest and widest available option on the shelf when the outbreak started. Their availability does not equate to efficacy. They rely on other pieces of PPE to cover their many shortcomings.
N95 masks are not bulletproof: they require perfect fit. If they do not create an air-tight seal around the nose, then infected air will enter through the openings around the mask (the path of least resistance is preferred in fluid dynamics) instead of passing through the filter.
The eyes also remain exposed, leaving another important entry point at risk. Face shields do block droplets and aerosols from the eyes.
Personal Air Purifier Systems (PAPRs) provide facial and respiratory protection, but these were not designed for Infectious Disease use but instead for industrial applications like silica dust. Users complain of heat, noise, and comfort, maintenance is a challenge given the many exposed reusable parts, and they were found to be so bad in doffing in Toronto in 2003 that the Ontario nurses threatened to strike if forced to use them.
Doffing is a distinguishing line between good and bad Infectious Disease PPE. There is no point in wearing PPE if the doctor or nurse gets infected removing it. Does the apparel help the wearer doff? Does it inform the user which surfaces were exposed and which were not? Does the wearer have to remove a second infected glove with a bare hand? Is the doffing simple and easy to execute? The CDC summarizes: "The manner in which the clothing is donned and doffed in sequence with other PPE is an important consideration when selecting gowns and coveralls. This is critical because the ease or difficulty with which PPE is put on and removed may affect its effectiveness and the potential for self-contamination, especially during doffing of contaminated PPE. Donning and doffing features included in the selection process should consider the entire PPE ensemble, not simply the gown or coverall."